
Dr. Abene is a board certified Orthopaedic Surgeon. He did his Sports Medicine Fellowship at Stanford where he worked directly with the head team physicians for the San Francisco 49ers and Giants. He is currently the head team physician for the San Jose Sharks AHL affiliate, the San Jose Barracuda. He is also a volunteer team physician for USA Hockey.
What Is The ACL?
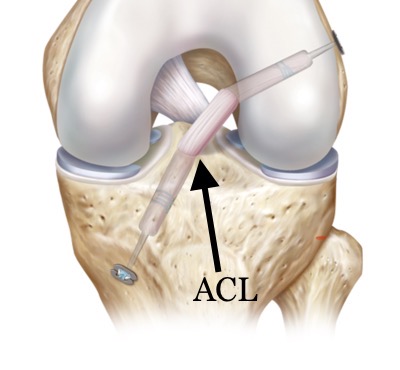
ACL stands for Anterior Cruciate Ligament of the knee. It is called a cruciate because it crosses another ligament, the Posterior Cruciate Ligament (PCL), to form an X directly in the middle of the knee joint. Cruciate comes from Latin and means “cross”. The knee is the largest and most complex joint in the body. It depends on four (major) ligaments and other muscles and tendons to function properly. There are two ligaments on the sides of the knee: The Medial Collateral Ligament (MCL) and the Lateral Collateral Ligament (LCL), along with the two cruciates in the middle. The ACL is about 1.5 inches long and attaches the lower leg to the upper leg. It is the major stabilizing ligament in the knee. It prevents the lower leg from moving forward, especially when making fast cuts on the ice and when battling in the corner.
How Is the ACL Injured?
One of the ways for the ACL to be injured is by a direct blow to the knee. Most ACL tears, however, happen without contact between the knee and another object. Hockey is different than sports in terms of these injuries due to the ice. Hockey players do not injure the ACL the same way football or basketball players do. Those players normally twist on a planted leg (due to cleats) or land awkwardly from a jump. Hockey ACL injuries typically happen when the skate is stuck along the boards or when an opposing player lands directly on the knee.
What Are the Signs Of An ACL Tear?
In many cases, when the ACL is torn, the player will feel the knee give way with an audible “pop”. The injury is usually associated with a moderate amount of pain and continued play is usually not possible. These guys are usually carried or assisted off the ice. Over the next several hours, the knee becomes very swollen and even walking becomes difficult.
How Is an ACL Tear Diagnosed?
The best time to examine the knee is shortly after the injury. Most team docs will perform a “Lachman” test to determine if the ACL is torn. The “Lachman” involves holding the thigh with one hand and trying to slide the rest of the leg forward with the other. A good team doc can usually make the diagnosis immediately but will also order an MRI for confirmation
What is an MRI?
MRI (magnetic resonance imaging) is a modern diagnostic imaging technique that produces cross-sectional images of the body. Unlike CT scans or X-rays, MRI works without radiation. Instead, the MRI uses magnetic fields and a sophisticated computer to take high-resolution pictures of bones and soft tissues. The MRI also gives more detailed information than a physical exam, such as whether there are other structures injured such as the meniscus. The MRI can also help determine the severity of the injury.
Does it require surgery?
The ACL usually does not heal on its own. In the 70’s and 80’s, before surgery was a good option, people who tore their ACL often lived with what everyone described as a “trick” knee. This often meant the end of a professional career, especially in cutting sports. It can be difficult to play hockey on an unstable, “ACL-less” knee. Nearly all players today elect to have the surgery.
Why can’t they just brace it?
Bracing of unstable knees and reconstructed knees has been traditionally thought of as beneficial. Unfortunately, the benefit appears to be more limited when looked at carefully and under strict testing conditions in the lab. Virtually all braces fail to control the critical 3-5 millimeters of motion that would be required to prevent a re-injury. Still, some form of light bracing may offer players some degree of enhanced stability, even if only through complex feedback mechanisms that the brain uses to help control the knee and the surrounding muscles.
What does the surgery involve?
The ACL tear can’t just be sewn together. It needs to be reconstructed with a graft. There are two types of graft: Autograft and Allograft. Autograft is harvested from the players own knee and is either taken from the hamstring tendons or from the front of the knee (bone-patellar tendon-bone (BPTB) graft). Allograft comes from a cadaver (dead guy) and can be an Achilles tendon or other tissue. Most of the docs in the NHL use autograft BPTB as this is still considered the “gold standard”. Once the graft is chosen the knee is scoped to look for other problems (meniscal tear, cartilage damage, etc.) and to prepare the knee for the graft. Tunnels are drilled in the shin bone (tibia) and the thigh bone (femur) and the graft is pulled into these tunnels. It is then fixated with either screws or other types of devices. The rehab begins immediately.
Return to Play?
This is a tough question to answer. Most Orthopods recommend a minimum of 6 months after the surgery prior to returning to full play but is usually between 8 months and a year. This timeline applies to almost everyone. Professional athletes, however, have access to state-of-the-art rehab and can somewhat shorten this time frame, but not dramatically. If a player returns too early, they can end up with a re-injury or other problems. While a player usually can return to the field in less than one year, there is a belief that it usually takes about 2 years, to fully recover from an ACL reconstruction. There is good data to back this theory up. The reasons for this are as much about the mental aspects of the game as they are the success of the surgery.
The contents of Neutral Zone and Dr Abene’s articles such as text, graphics, and images are for informational purposes only. The content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified healthcare provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something on the Neutral Zone website.
If you think you may have a medical emergency, call your doctor or 911 immediately. Neutral Zone does not recommend or endorse any specific tests, physicians, products, procedures, opinions, or other information that may be mentioned on the site. Reliance on any information provided by Neutral Zone, Dr Abene or any of its employees or other information appearing on the site is solely at your own risk.

